The Cosmetic Motivations Questionnaire (CMQ, Pikoos & Buchanan, 2022) is designed to help cosmetic professionals understand their patient’s core motivations and reasons for seeking cosmetic treatment.
The questionnaire involves a list of 27 common motivations for seeking cosmetic treatment which has been developed through an extensive review of the literature, and motivations for cosmetic procedures described in several quantitative and qualitative research studies (Maisel et al., 2018; Liew et al., 2019; Maisel et al., 2018; McDonald et al., 2022; Pikoos et al., 2021; Waldman et al., 2019).
Patient motivations are characterised according to the patient archetypes (Beautification, Transformation, Positive Ageing and Correction) that were identified by Liew and colleagues (2019) as key groups seeking cosmetic procedures. An additional ‘Emotional’ archetype has been added indicating that the primary reasons for undertaking the procedure are for psychological or emotional motives.
Results from the CMQ advise a practitioner about their patient’s reasons for undertaking the procedure, and provide recommendations and treatment considerations which can guide the consultation with these types of patients. In turn, this can help the practitioner to personalise their approach, increasing the likelihood of a satisfied patient. This can also help a cosmetic practitioner quickly gather information to determine the appropriateness of the patients’ motivations for treatment, as per their requirements under the Australian Medical Board Guidelines (2023) for patient assessment.
Validity and Reliability
The Cosmetic Motivations Questionnaire involves a list of 27 common motivations for seeking cosmetic treatment which has been developed through an extensive review of the literature, and motivations for cosmetic procedures described in several quantitative and qualitative research studies (Maisel et al., 2018; Liew et al., 2019; Maisel et al., 2018; McDonald et al., 2022; Pikoos et al., 2021; Waldman et al., 2019).
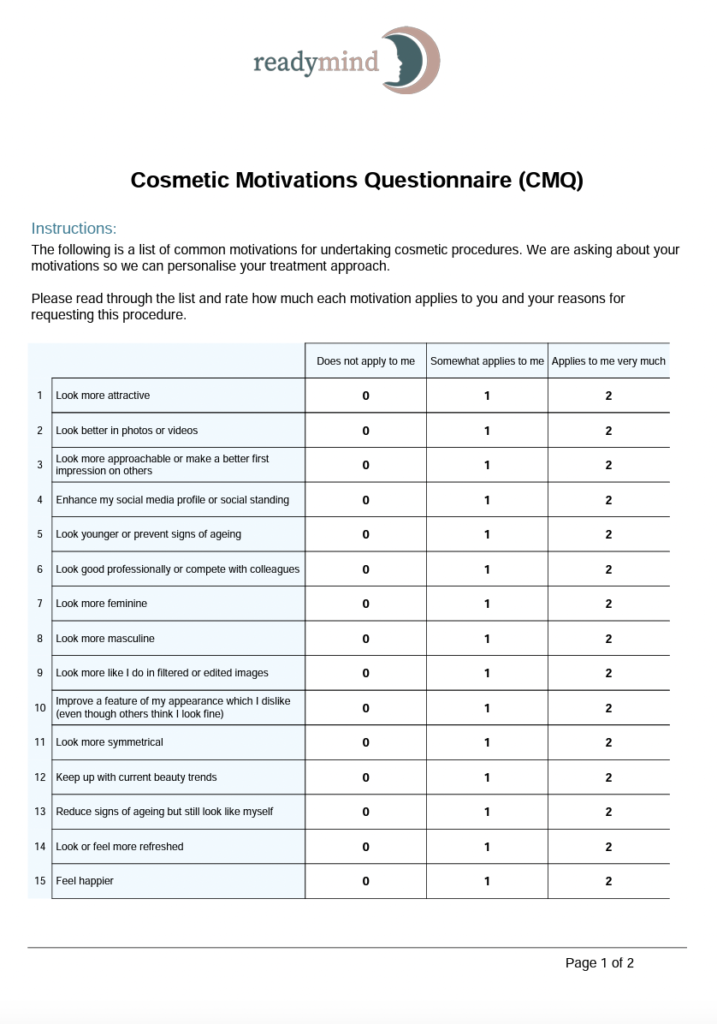
The list is designed to be comprehensive and covers the most common motivations expressed by patients, but is not exhaustive. Each motivation is scored on a 3-point Likert scale from ‘does not apply to me’ to ‘applies to me very much’.
Motivations for undergoing cosmetic procedures are often categorised as intrinsic or internal reasons, such as improving self-confidence, and extrinsic or external reasons, like pleasing a partner. Past research has found that individuals who are motivated for intrinsic (rather than extrinsic) reasons are more likely to be satisfied with the outcomes of a cosmetic procedure (Honigman et al., 2004; Sobanko et al., 2015; Maisel et al., 2018) Further, improvements in confidence and self-esteem following cosmetic treatment are more reliably reported than improvements in job prospects, social or romantic relationships (Castle, Honigman & Phillips, 2002; von Soest et al., 2009; Nair & Baboo, 2017; Pikoos et al., 2021). Therefore, external motivations may increase the likelihood that a patient has unrealistic expectations for the treatment.
The patient archetypes characterised by the Cosmetic Motivations Questionnaire were established by Liew and colleagues (2019) as part of the ‘Going Beyond Beauty’ initiative which incorporated 27 market research projects. The results were stratified into patient archetypes using segmentation analysis and then validated using online surveys, individual interviews and focus groups. A board of international aesthetic clinicians integrated the data with their own insights to characterise each archetypes. Data from over 54 000 participants in 17 different countries were distilled into four distinct patient archetypes based on motivating factors, aesthetic goals, initial treatment requests, and treatment opportunities and challenges. These archetypes were named Beautification, Positive Aging, Transformation, and Correction.
The authors mention that patients who have underlying psychological concerns such as body dysmorphic disorder (BDD) may fit into several of the four categories above (Liew et al., 2019). As such, for the CMQ, we have created a separate ‘Emotional’ category which detects motivations that have been associated with the presence of mental health concerns such as BDD, anxiety, depression and trauma in our pilot research (Pikoos & Buchanan, unpublished data). This category is designed as a prompt for the cosmetic practitioner to explore the patient’s psychological wellbeing in greater depth before performing a cosmetic treatment. Other measures available to support this include the Cosmetic Readiness Questionnaire, Cosmetic Procedure Screening Questionnaire (COPS), BDD Questionnaire – Aesthetic Surgery (BDDQ-AS).
Scoring and Interpretation
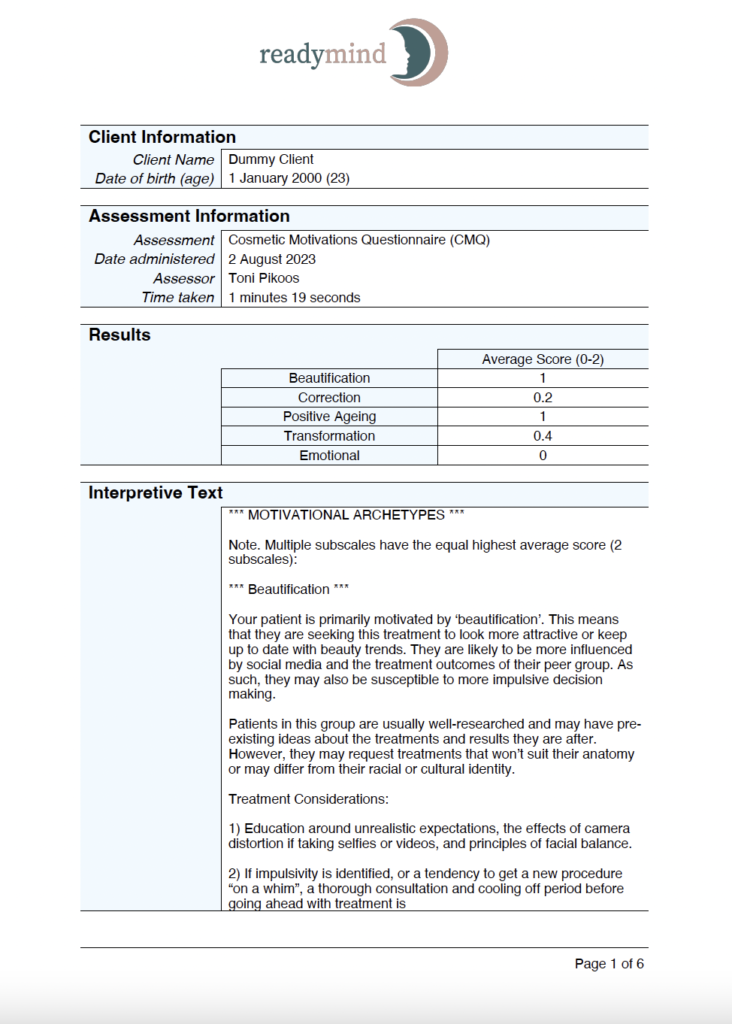
Each motivation is scored from 0 (does not apply to me) and 2 (applies to me very much). The items relating to each subscale are summed and averaged to produce an “average score”, which indicates the average response on the Likert scale. Higher scores indicate greater identification with that motivational archetype.
The subscales are as follows:
1. Beautification: This describes a patient who is primarily motivated by enhancing their physical attractiveness, or keeping up to date with beauty trends.
2. Correction: This describes a patient who is primarily motivated by correcting insecurities, or fixing a ‘defect’ in their physical appearance. This could be a perceived or visible feature in their appearance.
3. Transformation: This describes a patient who is eager for more drastic changes through cosmetic treatment. They may be hoping for professional, romantic or social changes after the procedure, or be seeking to alter their gender or racial identity through treatment.
4. Positive Ageing: This describes a patient who is primarily motivated by reducing signs of ageing or slowing down the progression of ageing. They often want natural results and to preserve their existing look.
5. Emotional: This describes a patient who may have emotional or psychological reasons for undertaking the procedure, such as a perceived flaw in their physical appearance, or a history of trauma or bullying which contributed to their treatment interest.
The subscale with the highest average score is considered to be the patients’ primary motivational archetype and results are presented accordingly.
If the patient has more than 3 equal maximum subscale scores, then only the first three archetypes are presented for ease of interpretation.
If the patient’s highest average score is less than 1 (so not a particularly high average score) then only one archetype is presented (regardless if there are multiple equal subscale average scores).
Developer
Pikoos & Buchanan, 2022
References
Honigman, Roberta J., Katharine A. Phillips, and David J. Castle. “A review of psychosocial outcomes for patients seeking cosmetic surgery.” Plastic and reconstructive surgery 113.4 (2004): 1229.
Liew, S., Silberberg, M., & Chantrey, J. (2020). Understanding and treating different patient archetypes in aesthetic medicine. Journal of Cosmetic Dermatology, 19(2), 296-302. Maisel, A., Waldman, A., Furlan, K., Weil, A., Sacotte, K., Lazaroff, J. M., … & Alam, M. (2018). Self-reported patient motivations for seeking cosmetic procedures. JAMA dermatology, 154(10), 1167-1174.
McDonald, C. B., Hart, S., Liew, S., & Heydenrych, I. (2022, January). The importance of patient mindset: Cosmetic injectable patient experience exploratory study—Part 1. In Aesthetic Surgery Journal Open Forum (Vol. 4, p. ojac043). US: Oxford University Press.
Nair, B. P., & Baboo, G. (2017). Effect of cosmetic surgery on body image and body image specific quality of life. Journal of the Indian Academy of Applied Psychology, 43(1), 157.
Pikoos, T. D., Rossell, S. L., Tzimas, N., & Buzwell, S. (2021). Assessing unrealistic expectations in clients undertaking minor cosmetic procedures: the development of the aesthetic procedure expectations scale. Facial Plastic Surgery & Aesthetic Medicine, 23(4), 263-269.
Pikoos, T. D., Rossell, S. L., Tzimas, N., & Buzwell, S. (2021). Is the needle as risky as the knife? The prevalence and risks of body dysmorphic disorder in women undertaking minor cosmetic procedures. Australian & New Zealand Journal of Psychiatry, 55(12), 1191-1201.
Von Soest, T., Kvalem, I. L., Roald, H. E., & Skolleborg, K. C. (2009). The effects of cosmetic surgery on body image, self-esteem, and psychological problems. Journal of plastic, reconstructive & Aesthetic Surgery, 62(10), 1238-1244.
Waldman, A., Maisel, A., Weil, A., Iyengar, S., Sacotte, K., Lazaroff, J. M., … & Alam, M. (2019). Patients believe that cosmetic procedures affect their quality of life: an interview study of patient-reported motivations. Journal of the American Academy of Dermatology, 80(6), 1671-1681.